

Hypertrophic Cardiomyopathy - HCM I
Hypertrophic cardiomyopathy is characterized by marked thickening of the left heart wall, namely the interventricular septum, which is the wall in between the two chambers the heart (i.e. the septum is the wall that divides the heart ventricles into left and right). In hypertrophic cardiomyopathy the thickening of the cardiac muscle wall is usually not due to high blood pressure. In most patients it can interfere with the normal propulsion of blood out of the heart (left ventricular outflow tract obstruction), whereas in other patients the contraction of the cardiac wall is inadequate.
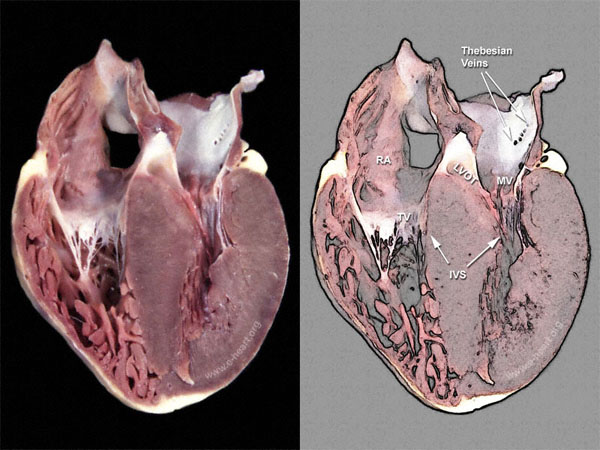
The most distinct gross examination finding in hypertrophic cardiomyopathy is the presence of asymmetric hypetrophy (thickening) of the interventricular septum when compared to the free wall of the left ventricle. There are three distinc types defined on the basis of the area of the interventricular septum that is most severely affected by the hypertrophy. 1. Basal type (this panel). 2. Mid-ventricular type. 3. Apical type.
The image shown in this panel is a four-chamber view of a heart showing biventricular hypertrophy. The left ventricle shows asymmetric septal hypertrophy with small ventricular cavity and contact of the anterior mitral leaflet with the septum. The hypertrophy is most severe towards the base (upper portion in the image)of the interventricular septum. The right ventricle is mildly dilated with hypertrophied trabeculae.
In some patients, specific inherited genetic defects have been identified that are responsible for the disease.
The histopathologic features of hypertrophic cardiomyopathy include myocyte disarray and small intramural coronary artery dysplasia.
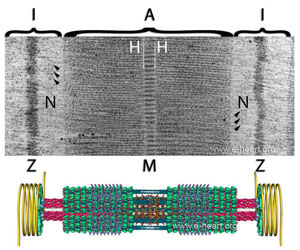
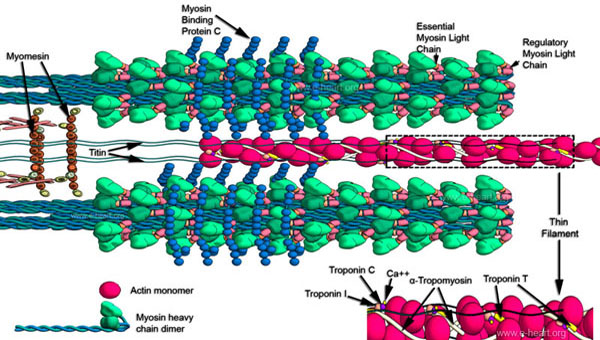
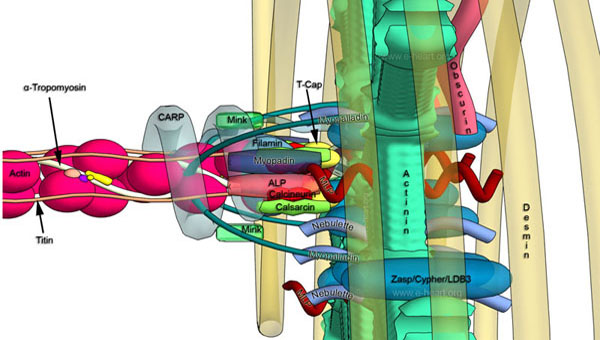
Genetic studies of HCM have shown mutations in sarcomeric genes and in non sarcomeric genes. The structure of the sarcomeres, the proteins that make up the thick and thin filaments and the thin filament to Z disc interface of the sarcomere is shown here. Some metabolic pathways that affect the lysosomes (LAMP2) or kinases (PRKAG2) involved in glycogen metabolism also produce a morphologic phenotype of HCM. In addition, amyloidosis and Fabry's disease are also mimickers of HCM.
{kind=link}
{kind=link}
{kind=link}