

Curriculum - Cardiomyopathies
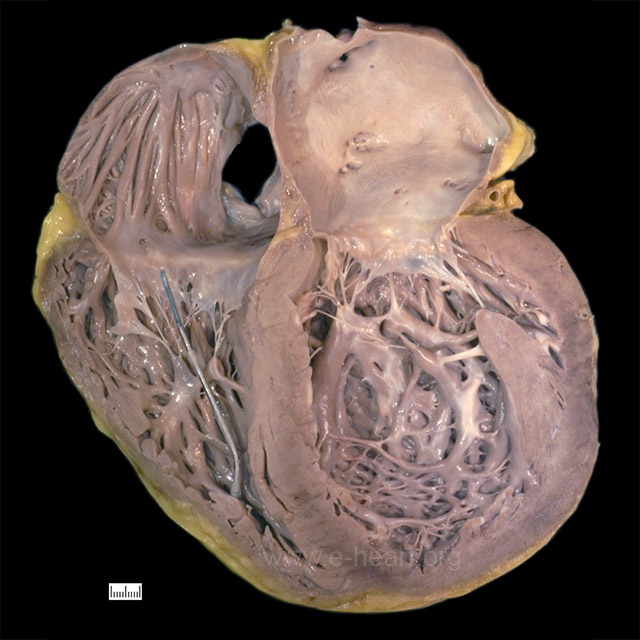 A case of dilated cardiomyopathy with enlargement of all four chambers, most severe in the left ventricle which appears globular. The wall thickness may be normal as the hypertrophy is masked by the dilatation. The right ventricle shows a segment of a pacing lead well anchored in the apex of this chamber.
A case of dilated cardiomyopathy with enlargement of all four chambers, most severe in the left ventricle which appears globular. The wall thickness may be normal as the hypertrophy is masked by the dilatation. The right ventricle shows a segment of a pacing lead well anchored in the apex of this chamber.
 This heart shows marked hypertrophy of the interventricular septum which is twice as thick as the left ventricular free wall. There is dilatation of the other chambers as well with a white organizing thrombus in the right atrial appendage.
This heart shows marked hypertrophy of the interventricular septum which is twice as thick as the left ventricular free wall. There is dilatation of the other chambers as well with a white organizing thrombus in the right atrial appendage.
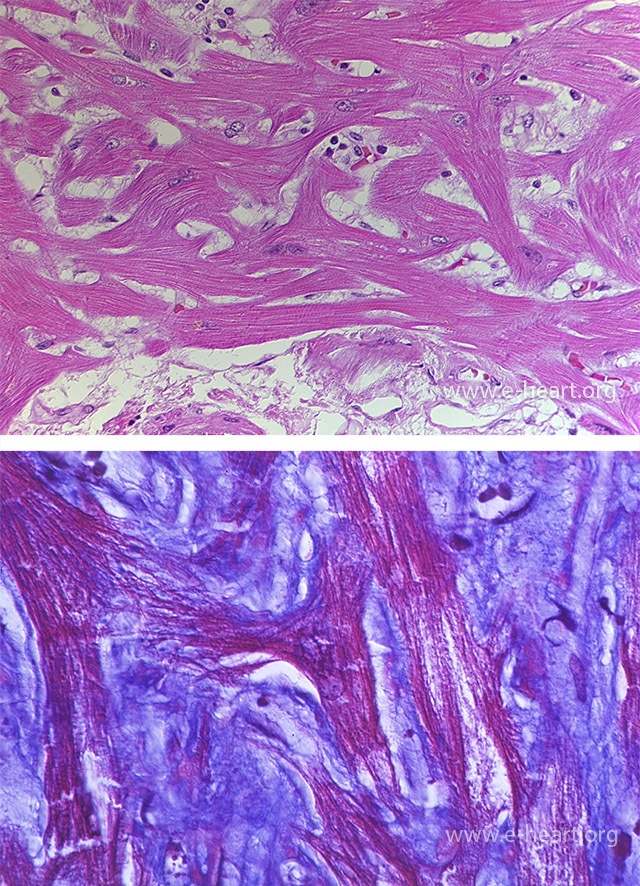 In hypertrophic cardiomyopathy, the hallmark of the disease is “disarray”. Disarray occurs at the fascicle level, myocyte level and sarcomere level. At the myocyte level, the myocyte sarcoplasm is disorganized forming branches in contrast to a normal parallel arrangement in sections taken from the interventricular septum. The disarray is also evident in the myofibrils within individual myocytes. This is often accompanied by interstitial fibrosis as shown in the trichrome stain.
In hypertrophic cardiomyopathy, the hallmark of the disease is “disarray”. Disarray occurs at the fascicle level, myocyte level and sarcomere level. At the myocyte level, the myocyte sarcoplasm is disorganized forming branches in contrast to a normal parallel arrangement in sections taken from the interventricular septum. The disarray is also evident in the myofibrils within individual myocytes. This is often accompanied by interstitial fibrosis as shown in the trichrome stain.
 The intramural coronary arteries in the septum of hearts with hypertrophic cardiomyopathy are often abnormal. The lumen is narrowed and the wall is thickened by an increase in the smooth muscle cells and ground substance in the media.
The intramural coronary arteries in the septum of hearts with hypertrophic cardiomyopathy are often abnormal. The lumen is narrowed and the wall is thickened by an increase in the smooth muscle cells and ground substance in the media.
 The outflow tract of the left ventricle in the obstructive type of hypertrophic cardiomyopathy shows endocardial thickening with fibrosis and elastosis evident in the Movat stain.
The outflow tract of the left ventricle in the obstructive type of hypertrophic cardiomyopathy shows endocardial thickening with fibrosis and elastosis evident in the Movat stain.
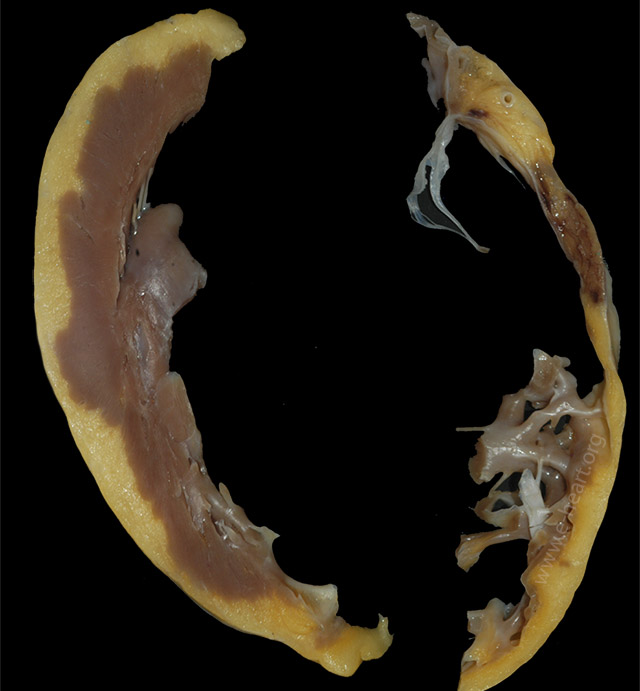
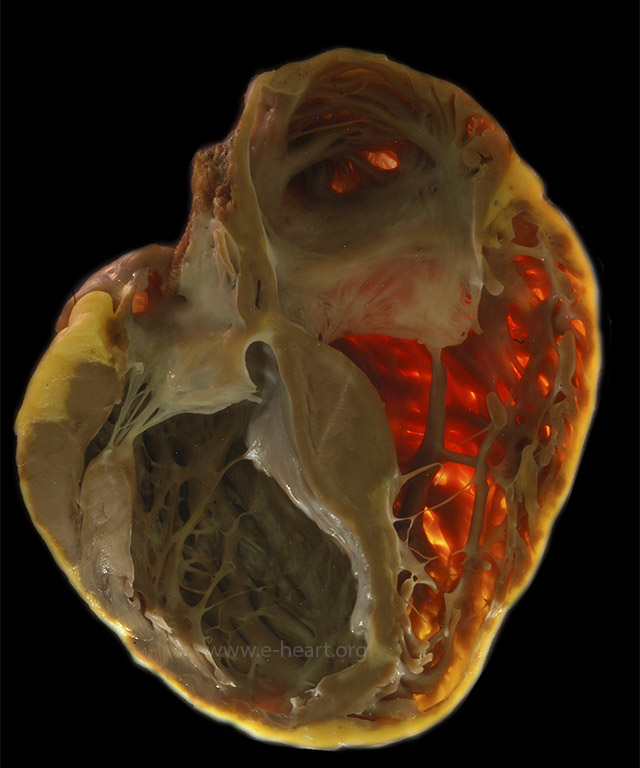 Transilluminated specimen shows loss of the compact zone in the right ventricle which appears translucent in a case of arrhythmogenic right ventricular cardiomyopathy. Also note the thinning of the left ventricular wall and interventricular septum towards the apex due to fibrofatty replacement.
Transilluminated specimen shows loss of the compact zone in the right ventricle which appears translucent in a case of arrhythmogenic right ventricular cardiomyopathy. Also note the thinning of the left ventricular wall and interventricular septum towards the apex due to fibrofatty replacement.
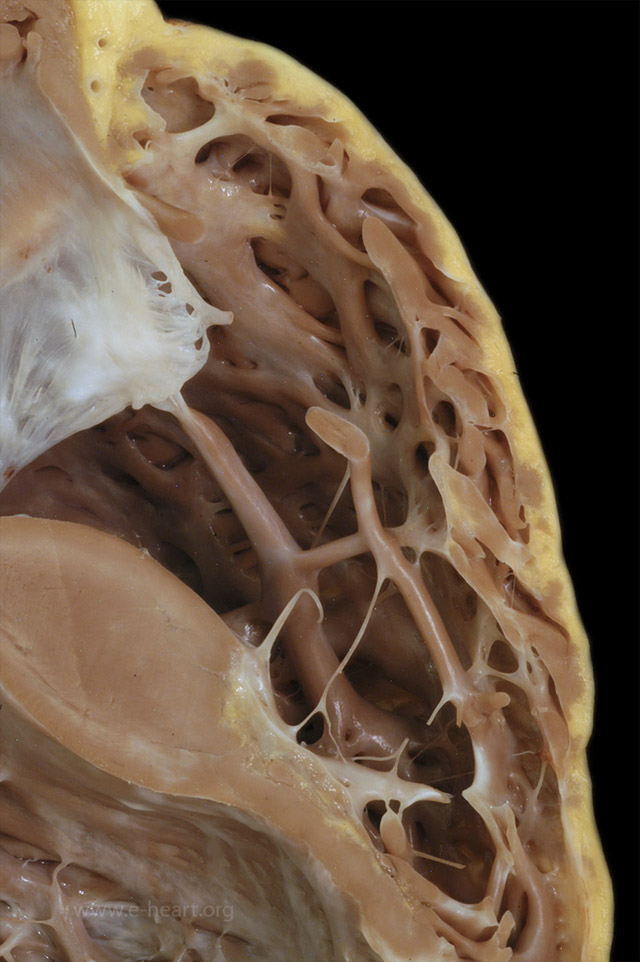 The right ventricular wall of the same heart in Figure 27.23 is shown. The compact zone is discontinuous with fatty infiltration and fibrous replacement. The trabecular myocardium is relatively spared.
The right ventricular wall of the same heart in Figure 27.23 is shown. The compact zone is discontinuous with fatty infiltration and fibrous replacement. The trabecular myocardium is relatively spared.
 In addition to the marked thinning of the wall of the right ventricle (shown on the right) due to fibrofatty replacement in arrhythmogenic right ventricular cardiomyopathy, involvement of the left ventricle with fatty infiltration producing a “moth eaten” appearance is seen in almost half of the cases. Note the irregular contour of the subepicardium of the left ventricle in this example.
In addition to the marked thinning of the wall of the right ventricle (shown on the right) due to fibrofatty replacement in arrhythmogenic right ventricular cardiomyopathy, involvement of the left ventricle with fatty infiltration producing a “moth eaten” appearance is seen in almost half of the cases. Note the irregular contour of the subepicardium of the left ventricle in this example.
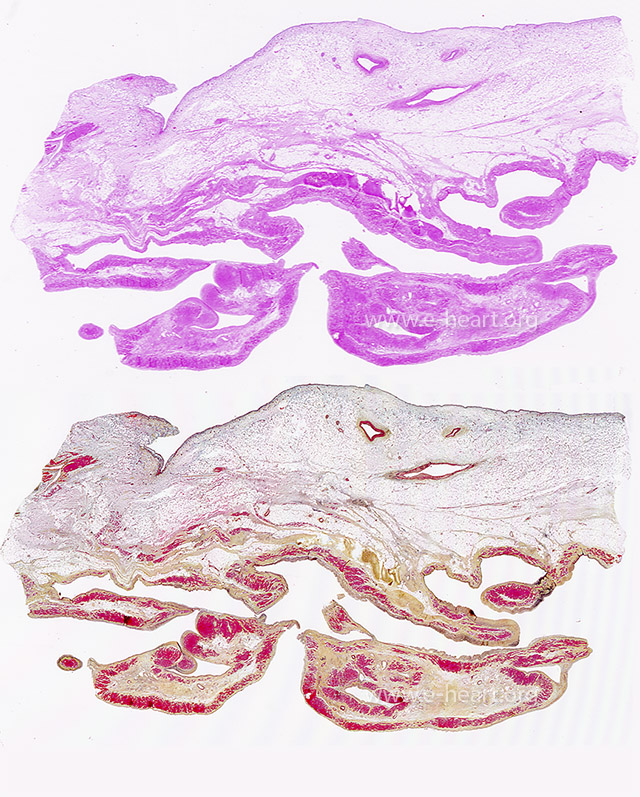 Section of the right ventricular wall with extensive adipose tissue replacement of the compact zone and trabecular myocardium as shown in an H&E stain and corresponding Movat stain. The Movat stain highlights the fibrous tissue in yellow.
Section of the right ventricular wall with extensive adipose tissue replacement of the compact zone and trabecular myocardium as shown in an H&E stain and corresponding Movat stain. The Movat stain highlights the fibrous tissue in yellow.
 The atria are enlarged and the endocardium of both atria shows fine yellow-ochre granular surface due to amyloid deposition. These deposits are also seen in the tricuspid and mitral valves leaflets.
The atria are enlarged and the endocardium of both atria shows fine yellow-ochre granular surface due to amyloid deposition. These deposits are also seen in the tricuspid and mitral valves leaflets.
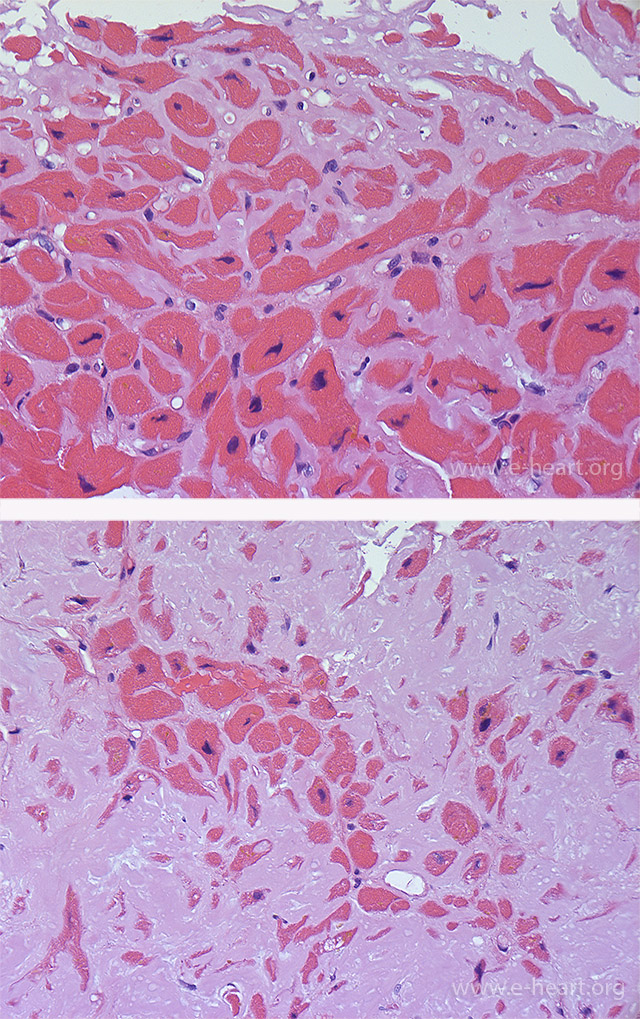 Amyloid infiltration in the heart shows “amorphous” eosinophilic material accumulating in the extracellular space. The amyloid is deposited thoughout the interstitium surrounding individual myocytes (top panel). In advanced disease, there is more pronounced myocyte atrophy with accumulation of the interstitial deposits into a nodular pattern (bottom panel).
Amyloid infiltration in the heart shows “amorphous” eosinophilic material accumulating in the extracellular space. The amyloid is deposited thoughout the interstitium surrounding individual myocytes (top panel). In advanced disease, there is more pronounced myocyte atrophy with accumulation of the interstitial deposits into a nodular pattern (bottom panel).
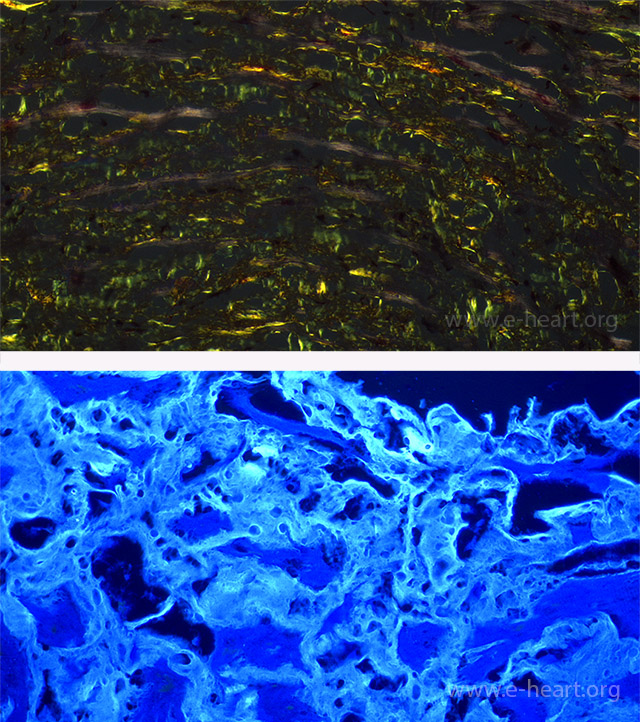 Interstitial amyloid shows apple green birefringence on polarization microscopy (top panel) when stained with Congo Red. Amyloid deposits also appear fluorescent with thioflavin S or T staining viewed under fluorescence microscopy. This is a more sensitive and reproducible stain than Congo Red.
Interstitial amyloid shows apple green birefringence on polarization microscopy (top panel) when stained with Congo Red. Amyloid deposits also appear fluorescent with thioflavin S or T staining viewed under fluorescence microscopy. This is a more sensitive and reproducible stain than Congo Red.
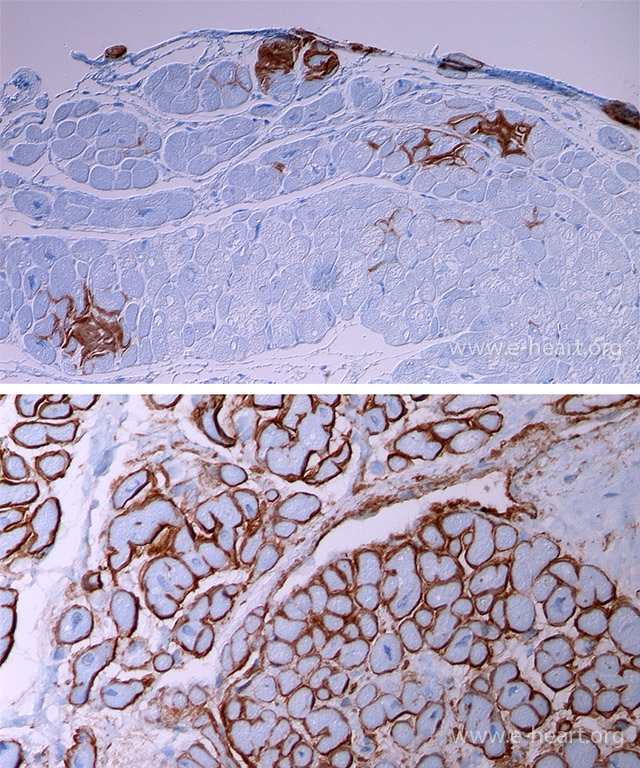 Immunohistochemical staining is useful for typing of cardiac amyloidosis. The top panel shows focal deposits of transthyretin in a coarse interstitial pattern and forming small nodules. The bottom panel shows a diffuse interstitial perimyocytic pattern of deposition in light chain amyloidosis where lambda light chains are at least twice as frequently seen compared to kappa light chain deposition.
Immunohistochemical staining is useful for typing of cardiac amyloidosis. The top panel shows focal deposits of transthyretin in a coarse interstitial pattern and forming small nodules. The bottom panel shows a diffuse interstitial perimyocytic pattern of deposition in light chain amyloidosis where lambda light chains are at least twice as frequently seen compared to kappa light chain deposition.
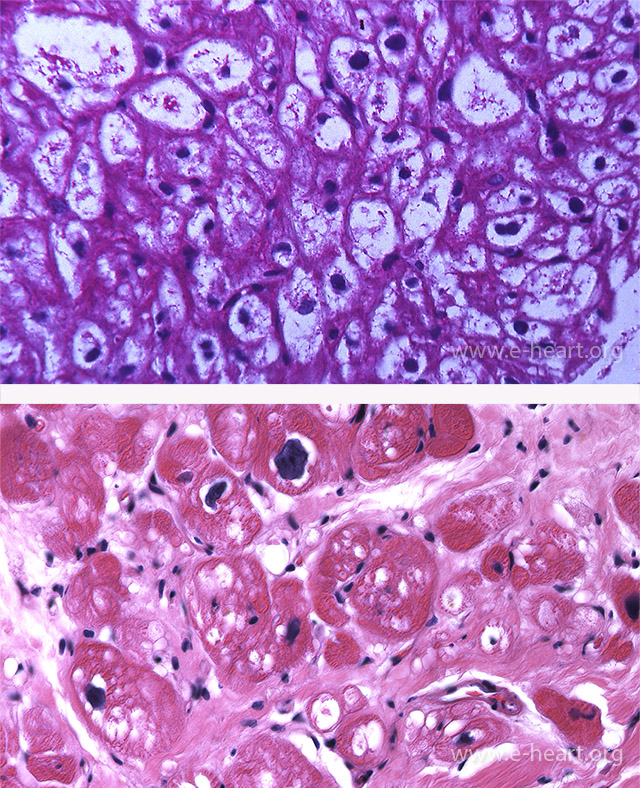 The myocytes are enlarged with pale sarcoplasm due to massive accumulation of glycogen that stain PAS-positive in a case of Pompe disease (top panel). In the adult, glycogen storage disease may appear as irregular vacuoles associated with interstitial fibrosis (bottom panel).
The myocytes are enlarged with pale sarcoplasm due to massive accumulation of glycogen that stain PAS-positive in a case of Pompe disease (top panel). In the adult, glycogen storage disease may appear as irregular vacuoles associated with interstitial fibrosis (bottom panel).
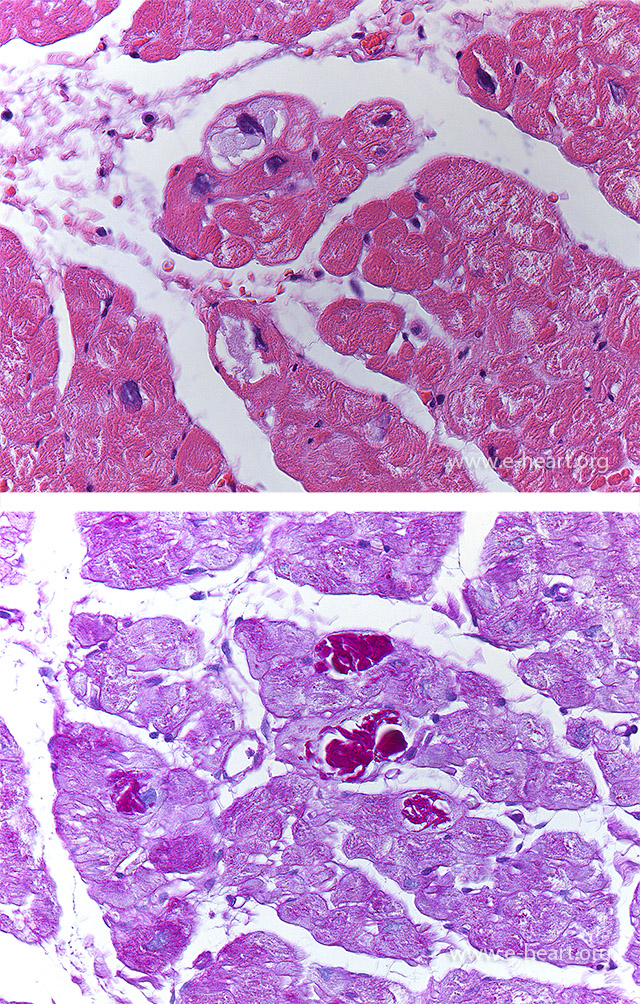 A few myocytes show accumulation of basophilic material in the sarcoplasm that is intensely positive with PAS. This type of glycogen deposition can be seen in type IV glycogen storage disease and in hearts of patients older than 65 years of age (basophilic degeneration).
A few myocytes show accumulation of basophilic material in the sarcoplasm that is intensely positive with PAS. This type of glycogen deposition can be seen in type IV glycogen storage disease and in hearts of patients older than 65 years of age (basophilic degeneration).
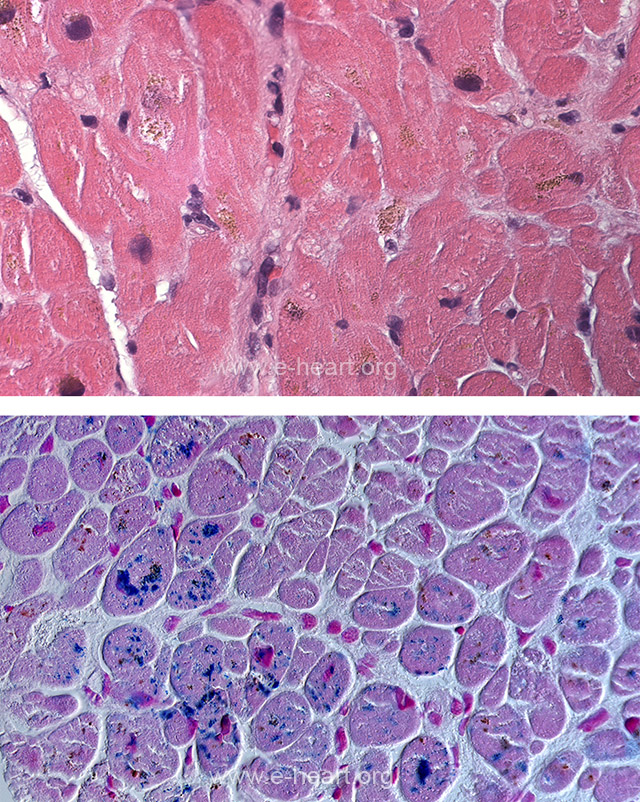 The myocytes contain dark-yellow-to-brown granular deposits mostly in perinuclear location (top panel) which are readily identified as iron on a Prussian blue stain (bottom panel) in a case of hemosiderosis.
The myocytes contain dark-yellow-to-brown granular deposits mostly in perinuclear location (top panel) which are readily identified as iron on a Prussian blue stain (bottom panel) in a case of hemosiderosis.
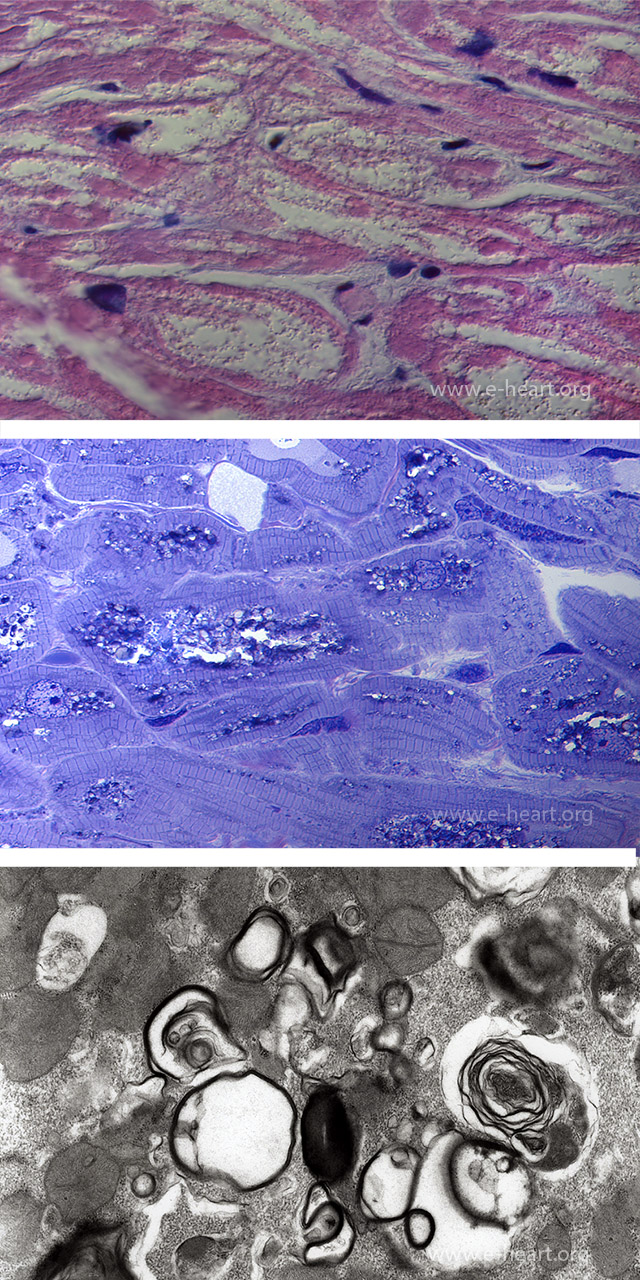 In Fabry disease, there is marked vacuolation of the myocytes. The myofibrils are displaced to the periphery by the deposits occupying the central clear to finely granular area (top panel). On toluidine blue stain of a semithin section, the glycolipid deposits are evident as dark blue metachromatic deposits in Touluidine blue stained plastic section. Ultrastructural examination demonstrates that the metachromatic deposits are in fact the characteristic lamellar bodies seen in Fabry’s disease.
In Fabry disease, there is marked vacuolation of the myocytes. The myofibrils are displaced to the periphery by the deposits occupying the central clear to finely granular area (top panel). On toluidine blue stain of a semithin section, the glycolipid deposits are evident as dark blue metachromatic deposits in Touluidine blue stained plastic section. Ultrastructural examination demonstrates that the metachromatic deposits are in fact the characteristic lamellar bodies seen in Fabry’s disease.
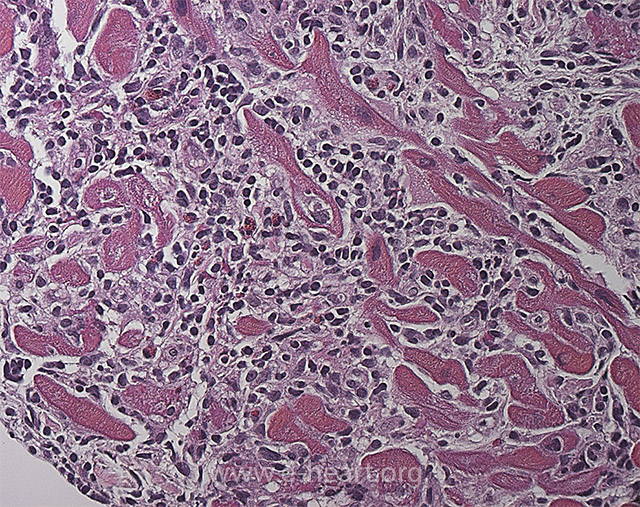 Lymphocytic myocarditis showing dense infiltrates of lymphocytes, histiocytes and few eosinophils that expands the interstitial space. Myocyte injury is evident in the left lower corner of the field showing fragmentation and irregular borders of the myocytes.
Lymphocytic myocarditis showing dense infiltrates of lymphocytes, histiocytes and few eosinophils that expands the interstitial space. Myocyte injury is evident in the left lower corner of the field showing fragmentation and irregular borders of the myocytes.
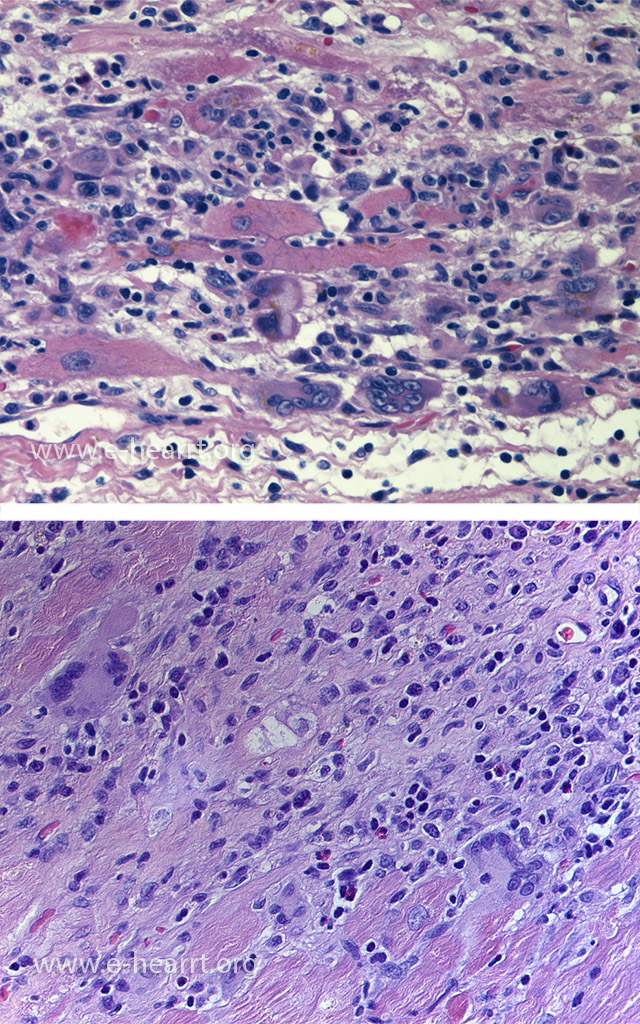 Giant cell myocarditis showing an aggressive inflammatory infiltrate notable for the presence of multinucleated giant cells and variable amount of eosinophils in both images. Well-formed granulomas are absent.
Giant cell myocarditis showing an aggressive inflammatory infiltrate notable for the presence of multinucleated giant cells and variable amount of eosinophils in both images. Well-formed granulomas are absent.
 A case of cardiac sarcoidosis with marked biventricular dilatation of the heart. There is sclerotic white “waxy” appearing formation of scars in the interventricular septum and posterior right ventricular wall. Mural thrombi are present in the right ventricle.
A case of cardiac sarcoidosis with marked biventricular dilatation of the heart. There is sclerotic white “waxy” appearing formation of scars in the interventricular septum and posterior right ventricular wall. Mural thrombi are present in the right ventricle.
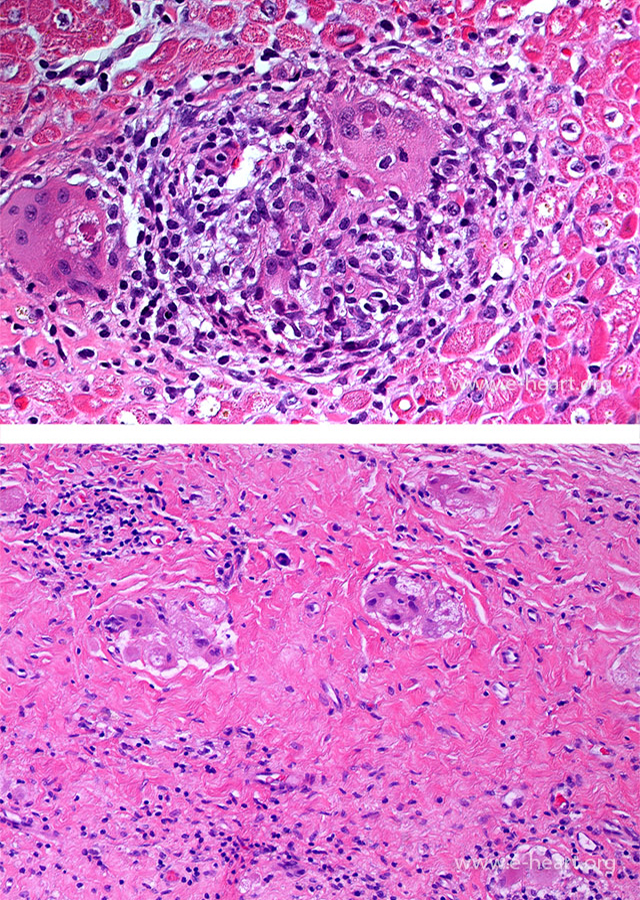 Cardiac sarcoidosis showing discrete non-necrotizing granuloma in the myocardium (top panel). Small granulomas and multinucleated giant cells typically persist within dense fibrosis in areas of gross scarring (bottom panel).
Cardiac sarcoidosis showing discrete non-necrotizing granuloma in the myocardium (top panel). Small granulomas and multinucleated giant cells typically persist within dense fibrosis in areas of gross scarring (bottom panel).